 |
MGH Community News |
|
MGH Community News |
| October 2014 | Volume 18 • Issue 10 |
Highlights
Sections Social Service staff may direct resource questions to the Community Resource Center, Lindsey Streahle, x6-8182. Questions, comments about the newsletter? Contact Ellen Forman, x6-5807. |
Fuel Assistance Season Begins November 1 It’s that time of year again. Fuel Assistance (the Low-Income Home Energy Assistance Program or LIHEAP) programs start accepting new referrals as of November 1. The MA Department of Housing and Urban Development (DHCD) has just increased the benefits a household can get under LIHEAP. The full table of eligibility and corresponding benefit levels, which vary by heating source and household income, can be found here: http://www.mass.gov/hed/docs/dhcd/cd/liheap/fy15liheap-incomeeligibilityandinitialbenefitlevels.pdf Utility Discounts This is also a good time to ensure that those eligible are receiving discounted utility rates where applicable as Fuel Assistance rarely covers all of one’s utility expenses. Investor-owned* utility companies (gas, electric, local phone) in Massachusetts must offer reduced rates (about 25% discount) to certain low-income households. The income guideline is the same as for Fuel Assistance (less than 60% area median income). One must also already receive some type of income-tested benefit. There are many low-income programs that can qualify a household for the utility discounts, including fuel assistance, TAFDC, SNAP (food stamps), school lunch, housing subsidies, and certain subsidized health care coverage programs. Some utility companies automatically enroll eligible customers; however if this is not the case, customers can apply. *Note that Municipal utilities (those owned by a city or town) are NOT required to offer discounts. The Winter Moratorium - Shut-Off Protection In Massachusetts utilities are prohibited from shutting-off heat-related utilities between November 15 and March 15 each year (commonly extended a few weeks on an annual basis) for those with documented “financial hardship”. This protection applies only to gas and electric utilities, and not to “deliverables” such as oil, propane, kerosene and wood. It does apply to electricity in homes that heat with gas if electricity is required to operate the heating system. To qualify, one must document “financial hardship” by completing a utility-specific form and supplying required additional documentation. While the winter moratorium provides protection from shut-off during this time period, it does not erase the debt. Utilities are free to, and often will, proceed with shut-off at the end of the moratorium unless arrangements are made to address overdue bills. |
Mass Rental Voucher Program Waitlist Lottery Open Through Nov 3 (While many readers received an earlier version of this story in a 10/15 e-mail, additional information and an important new advocacy tip have been added to this version.) The state has recently made available funding for a limited amount of new Massachusetts Rental Program (MRVP) mobile vouchers. MRVP mobile vouchers provide rental assistance to low-income families and individuals who lease privately-owned apartments. A household pays at least 30 percent, but not more than 40 percent, of its income as rent plus any tenant-paid utilities. Housing agencies must first establish a waiting list from which applicants, who apply and are randomly assigned to the waiting list, will be selected to be screened for eligibility. Six of the regional housing agencies will be accepting MRVP applications for this lottery from Monday, October 6, 2014 to Monday, November 3, 2014. All applications must be received or postmarked no later than 5 p.m. on Monday, November 3, 2014. The Mass Coalition for the Homeless is recommending that families and individuals apply to all six lists to maximize their chances of being selected for one of these currently available subsidies and for subsidies that may become available in the future. AND if homeless*, ALSO use the *Homeless applicants may be eligible for a priority. They need to complete two applications- the Universal STANDARD application and the Universal Emergency application. (See the Emergency application for the definition of “homeless”.) Submit completed applications, either in person or by mail, to the appropriate regional agency. No applications will be accepted by fax or email. Applications are being accepted until 5 p.m. on November 3, 2014. All timely applications will be entered into a lottery to determine waiting list placement. Application date will not affect placement on the waiting list. Please see each agency websites for specific income limits and additional information related to submitting applications. Community Teamwork, Inc. Housing Assistance Corp. HAPHousing Metropolitan Boston Housing Partnership RCAP Solutions, Inc. South Middlesex Opportunity Council Also see accompanying story on housing options for homeless families. -Adapted in part from Help Spread the Word: Certain MRVP Housing Subsidy Waiting Lists Have Been Re-Opened Until 11/3!, Kelly Turley, Mass Coalition for the Homeless, October 22, 2014. TAFDC Expands Pregnant Teen Eligibility As previously reported (New Mass Welfare Law, MGH Community News, July 2014), a new state law made a variety of changes to the TAFDC and EAEDC programs. We recently became aware of another provision not widely reported at the time. Otherwise eligible pregnant teens are now eligible for their entire pregnancy if they meet the school attendance requirements. Previously they, like pregnant adults, were only eligible for the last 120 days of their pregnancies (determined by their due dates).
This provision went into effect with the issuance of Operations Memo 2014-59 on September 18, 2014. -Thanks to Kelly Turley of the MA Coalition for the Homeless for her assistance with this article. SNAP Business Process Redesign - Move to First Available Worker Model As of October 27, 2014 the Department of Transitional Assistance has moved from a case ownership model to a First Available Worker (FAW) Model for SNAP-only eligibility determination and case maintenance. Rather than operating under an individual caseload model, all SNAP-only activities will be distributed on a statewide basis to SNAP case managers. The FAW model is exclusive to SNAP-only households. Cash and combination cases will continue to be managed under the caseload ownership and TAO (Transitional Assistance Office) assignment model. Eligibility policies for the programs administered by DTA have not changed. Beginning October 27, 2014, individual SNAP case manager phone numbers will no longer be referenced on Department notices and communications. Notices will refer all clients (cash and SNAP) to the toll free phone number, 1-877-382-2363, the Department’s statewide Assistance Line. Callers to this number will first be engaged by the enhanced Interactive Voice Response (IVR) services system which will allow them to complete some routine tasks such as checking the status of an application, updating a mailing address, and requesting an Income Verification Letter. IVR services will be offered to clients in five languages: English, Spanish, Portuguese, Cantonese, and Vietnamese for most tasks. Effective October 27, 2014, SNAP case managers will no longer have assigned caseloads. All SNAP-only casework will be assigned on a statewide basis rather than by TAO catchment area. As there will be no case assignment in the SNAP program, multiple case managers, in multiple TAOs, may now play a role in a single eligibility determination. Clients will have a team of case managers assisting them rather than a single designated case manager. SNAP case managers will no longer have client voicemail messages to respond to. This will allow SNAP case managers more time to devote to casework activity, resulting in faster eligibility determination and benefit issuances for eligible clients. No Wrong Door – SNAP-only clients are never in the wrong office. While TAO catchment areas will still determine such factors as where appointments are scheduled for hearings and other in-office appointments, SNAP-only clients can conduct their business at the TAO of their choosing. Centralized SNAP/SSI Office Advocacy and Feedback -Adapted from DTA Operations Memo 2014-66, October 16, 2104 Harbor Bridge Closing Causes Boston Shelter & Detox Shortage In early October the aging two-lane bridge connecting Long Island in Boston Harbor to the mainland was abruptly declared too dangerous for vehicles to cross. The closure caused the city to order the evacuation of the island which housed about one-third of all Boston shelter beds (in the city’s largest homeless shelter) and about half the city’s detox beds. In the middle of an epidemic of overdoses, there were 135 detox beds in the city of Boston before the close and now there are just 75. Officials scrambled to find shelter for more than 400 homeless people and as many as 300 others in recovery programs. These programs are now in limbo and it could be as long as five years and cost some $90 million before the 64-year-old bridge is replaced. With winter approaching, social service providers throughout the city worried that the decision to close the city’s largest homeless shelter would have a major ripple effect on their already strained resources. In recent years, the shelter has housed nearly 600 people on the coldest nights of the year. The abrupt decision to close the bridge came on Wednesday October 9, when state inspectors, using new criteria to judge the reliability of bridges, determined that the rusting mass of steel plates, concrete, and rebar was no longer safe, even for the few vehicles allowed to cross. The bridge has been clearly deteriorating for quite some time. For years, a gate has blocked access to the span, with guards allowing only authorized vehicles, such as the buses that bring an average of 440 homeless people a night onto the island.
But city officials did not expect that it would have to be closed so suddenly. They said it became urgent to do so because the structural deficiencies mirrored those that caused a bridge over the Mississippi River in Minneapolis to collapse in 2007. -See the full Boston Globe coverage...
Housing Assistance- Review of Key MA Programs and How They are Faring in the New Fiscal Year Families at risk of losing their housing will be getting extra help from state programs designed to prevent homelessness this year, according to a top state housing official. Recent months have been tough for families on the verge of homelessness, Aaron Gornstein, undersecretary of the state Department of Housing and Urban Development, told members of the Cape & Islands Regional Network to Address Homelessness recently. Off-Cape, record numbers of families found their way into emergency shelter in motels and hotels last summer, Gornstein said. "We had a significant influx into the shelter system," a surge not seen in years, with 2,200 families in motels and hotels, Gornstein said. "The demand for emergency shelter is still very high," with 1,950 families remaining in hotels and motels. Housing organizations in the network — and their clients — will benefit from increased state funding this fiscal year for homeless prevention, said Gornstein. For one, the state has doubled the financial assistance available to families for the HomeBASE program to prevent homelessness.The stipends went from $4,000 to $6,000 in January then climbed to $8,000 July 1, the start of the fiscal year. HomeBASE is a one-time, short-term housing assistance program that helps people cover the cost of security deposits, furnishings, moving costs and rent, Gornstein said. The program is intended to divert people from emergency shelters and help other people out of shelters. Frederic Presbrey, head of the Hyannis-based Housing Assistance Corp., said, "$8,000 can really make the difference between being able to pay your rent or not." Another state homelessness prevention program, called RAFT — for Residential Assistance for Families in Transition — is getting an extra $1.5 million in funding this year. The increase brings the RAFT budget to $11 million. RAFT allows low-income families who are homeless or at risk of homelessness to get up to $4,000 in assistance over a 12-month period for expenses such as first and last month's rent, security deposits, overdue utility bills and work-related transportation expenses. "It's often used for back rent, getting caught up on utilities or moving expenses," Gornstein said. On average RAFT spends $2,500 to keep a family out of shelter, but paying for a family to stay in a shelter costs about $3,000 a month for an average stay of seven months, he said. In addition, the state is issuing 1,000 new rental vouchers to state housing authorities and other agencies that will help families and individuals move off waiting lists and into housing, Gornstein said. (See accompanying story for how to apply to the MRVP waitlist.) "There's huge waiting lists at every housing authority," he said. The rental voucher program has been expanding in the past few years, with a focus on moving people out of shelters. This is the first year the expansion will address waiting lists, Gornstein said. The rental vouchers work like Section 8 certificates, in that individuals and families get financial assistance to subsidize the cost of rent in the private market, Gornstein said. -See the full Cape Cod Online article... Consumer Alert- Electricity Competitive Suppliers: Read the Fine Print As reported previously (Consumer Alert- Electric Competitive Supplier Complaints, MGH Community News, February 2014), since the passage of Massachusetts’ electric utility Restructuring Act in 1997, electric customers are free to choose a "competitive supplier" for their electricity. Customers of National Grid, NSTAR Electric, Western Mass. Electric and Unitil/Fitchburg still have to pay those companies for distribution or delivery services (delivering the electricity to the customer's house, over the company's poles and wires), but the customer can purchase the actual electricity from a large number of licensed "competitive suppliers." Advocates are reporting an increase in marketing efforts from these companies who say they can beat National Grid’s currently high prices. Charles Harak, National Consumer Law Center (NCLC) attorney, in a post to the Utility Network Listserv, expresses concern with National Grid’s recent increase in prices, but stresses it is complicated to predict prices and what will benefit the consumer in the long run. Here’s an edited excerpt:
An advocate reported to NCLC that one competitive supplier requires a four-year contract with a $1,200 early termination fee! Consumers are advised to read the fine print! NCLC recently created a couple of information sheets about competitive suppliers:
-Adapted from e-mail statement from Charles Harak, NCLC attorney, to the utility network, utilitynetwork@lists.nclc.org, October 27, 2014
Naloxone Kit Available at MGH for Opioid Overdoses To help prevent opioid overdose deaths, any MGH patient now can request intranasal Naloxone without a prescription at the MGH Outpatient Pharmacy in Boston or Revere. Administered intranasally, Naloxone is an “opioid antagonist” prescription used to counter the effects of opioid overdose – which may instantly save a life. Anyone with an MGH medical record number can request the prescription for a family member, friend or loved one. Naloxone will be filled under a standing order – a physician’s order that can be exercised by other health care workers – and MGH pharmacists will provide training for its administration. “It is critical we create a simple pathway to increase access to this medication and use the expertise of our MGH pharmacists to ensure safe and timely administration,” says Christopher Fortier, PharmD, MGH chief pharmacy officer. MGH Pharmacy will bill the MGH patient’s insurance company under their MGH medical record number. Most insurance companies now pay for the kit, Fortier says. Explains Sarah Wakeman, medical director for Substance Use Disorders in the MGH Center for Community Health Improvement, “If I am an MGH patient, and I am concerned about my relative, I can ask the pharmacist for an intranasal Naloxone kit. The prescription will be in the name of the MGH patient as prescribed by the Commonwealth’s Good Samaritan law. The MGH patient can use the Naloxone on anyone.” According to Wakeman, Naloxone is safe, is non addictive and can be administered by any minimally trained individual. However, she stresses it is still crucial that emergency medical professionals are contacted for any overdose, since Naloxone does wear off, and individuals who experience overdose still require emergency medical attention. It may take multiple doses of Naloxone to revive someone who has overdosed on the deadly heroin/fentanyl combination. - MGH Hotline, October 3,2014.
Text4baby- Free Enhanced Text Messaging Service to Support Pregnant Women and New Mothers
As reported previously (Text4baby- Information for Pregnant Women and New Mothers, March 2012 MGH Community News), Text4baby, a program of Health Care For All’s (HCFA) HelpLine, offers free health and safety text messages three times a week throughout pregnancy and until baby turns one. Patients can sign up by texting BABY or (BEBE for Spanish) to 511411 on their cellphones. The Massachusetts Women, Infants and Children (WIC) Nutrition Program has been promoting Text4baby to participants since 2010. External evaluations of Text4baby have shown significant positive results.
Talking to Patients about Text4baby
Health care providers are critical partners in enrolling women in Text4baby. Given the limited How Text4baby Works Women who Text BABY (or BEBE for Spanish) to 511411 receive three weekly text messages timed to their due date or their baby's birth date up to age one.
- See the full MassHealth All Provider Bulletin 247, September 2014. Roca Antiviolence program Expands into Boston Using “Pay-for-Success” Contract For more than 25 years, Roca has served Greater Boston from its Chelsea headquarters. It is now putting down roots in the heart of Boston with a new facility in the shadow of the South Bay House of Correction, just off Melnea Cass Boulevard on Albany Street. Molly Baldwin, the founder and chief executive of the nonprofit, said the anti-violence program site is “somewhat neutral territory.” “We wanted to find a place where young people from different groups or gangs would feel comfortable coming to,” she said. Roca’s expansion into Boston started in January when it became the state’s first “pay-for-success” contract. The innovative financing tool, also referred to as a “social impact bond,” works like this: Philanthropists and commercial investors put up the money a program needs to expand, and the state pays them back if the program is successful. A program has five years to meet its goals, as determined by a third-party evaluator. “This is a very different model of government than paying now and asking questions later,” said Glen Shor, the state secretary of administration and finance. Roca started accepting young men into the program in January, when it became the program that pay-for-success, which is expanding to include housing and education, would be molded around. The program is working with 87 young men from Roxbury, Dorchester, Mattapan, Jamaica Plain, and the South End. Roca’s transitional employment program is built knowing the men will relapse — slip back into destructive behavior — and it focuses on relentless outreach and engagement to change behavior and find jobs. But once a young man opens the door or returns a call, the conversation doesn’t begin with lectures about avoiding jail time, breaking the cycle of poverty, or creating healthy relationships with family members. At first, youth workers say, there are kind gestures such as checking on the individual’s well-being to see if he needs anything — food, shelter, clothing — because most have dropped out of school, many are unemployed, and some are homeless. “The push for change is not immediate,” Torres said. “If we don’t have a relationship to bring them back after they relapse, then we’ve failed.” Roca workers Miguel Torres and Maria Amezquita said they want theirs to be the first number dialed in a time of need, whether it is for something serious like a young man having just been shot at and the urge for retaliation is irresistible, or something simple like needing light bulbs. Roca, which means rock in Spanish, is constantly crunching numbers to determine the progress of its young men as they make their way through the four-year program: Of those who had been there at least two years, 92 percent had no new arrests, 98 percent did not have a technical violation of their probation or parole, and 85 percent were employed for six months. -See the full Boston Globe article...
Mass Offers Medical Services Prices Online At one place, it costs $372. At another, $1,223. These are the prices members of Neighborhood Health Plan will pay out of pocket for the same procedure, an MRI of the lower back, at different health care providers. Neighborhood and other insurance companies have started posting such prices online, as required by a 2012 state law. State officials hope consumers will use the information to comparison shop for scans, colonoscopies, knee replacements, and other procedures just as they shop around for consumer products like furniture and appliances. The goal is to control health care costs by enticing consumers to choose care in lower-cost settings, and to nudge high-cost providers to reduce their rates to remain competitive. State officials kicked off an ad campaign this month to encourage consumers to research health care prices, with a new website, www.getthedealoncare.org. The site links to cost comparison tools for 13 insurers. Consumers already can call insurance companies to get price quotes, but as of Oct. 1, that information must also be online. Consumers can access only their own insurers’ prices. For example, a Harvard Pilgrim Health Care customer can’t see what the costs would be under a Blue Cross Blue Shield plan. The new cost estimators give consumers a list of all the doctors or health care facilities in a certain area that perform a certain service, from the lowest cost to the highest cost. The cost breakdown includes the amount paid by the consumer and the amount paid by the insurer. Each insurer’s website, however, varies. Some list many more procedures than others. The new price information comes at a time when high deductible health plans, which put a greater cost burden on consumers, are on the rise. The greater transparency around prices could put a spotlight on providers with the highest price tags. The Massachusetts Hospital Association said it supports the transparency measures but added that implementing such programs is complex. “It’s in the mutual interest of patients, providers, and insurers that this information is provided in an accurate and coordinated manner,” the association said. -See the full Boston Globe article...
MassHealth Inpatient Coverage – Now No 20-day Coverage Limitation Effective October 1, 2014, MassHealth now pays for inpatient services in acute inpatient hospitals beyond 20 days for members of all ages. Prior to this change, MassHealth would only pay for a maximum of 20 days of inpatient care for those 21 or over. This change should not be confused with the change to the MassHealth bed-hold which, as of September 1, 2014, is now 20 days; it was 10 days prior to that date (MassHealth Increases Bed-Hold Days to 20, MGH Community News, September 2014). Under the bed-hold, MassHealth will pay to retain the nursing home bed of MassHealth SNF residents who need acute hospitalization for a maximum of 20 days (formerly 10 days). -See the MassHealth, Transmittal Letter AIH-51, September 2014. Those with Insurance through The Connector- including MassHealth Temporary Coverage- Must Re-Enroll Temporary coverage is ending soon for individuals with temporary MassHealth coverage and those currently covered through Commonwealth Care. Beginning in November 2014, and continuing through December, MassHealth and the Massachusetts Health Connector will be sending these individuals call-to-action notices asking them to submit new applications for 2015 coverage before temporary MassHealth or Commonwealth Care coverage ends. Individuals with temporary MassHealth will receive notices between November 15th and December 15th. These members will have 60 days from the date of the notice they receive to take action before temporary coverage ends. Current Commonwealth Care members will receive notices on November 13th, 2014 and in order to avoid any gaps in coverage must submit a new application and enroll in new coverage by January 31, 2015. While Open Enrollment runs through February 15, QHP members will need to reapply and premium payments must be received by December 23, 2014 to avoid a gap in coverage. Our patients may contact Patient Financial Services for assistance, or beginning November 15 they may go online to www.mahealthconnector.org or call the Health Connector at 1-877-MA-ENROLL (1-877-623-6765). -Adapted from 2 Customer Service, Manage Claims and Payment Notices - Monday, October 20, 2014, MA Health Care Training Forum e-mail. Top Official Confident in Mass. Connector Website The top official overseeing the overhaul of the Massachusetts Health Connector’s website said early this month that he is “very confident” the software will work well when open enrollment starts Nov. 15. “We’re looking forward to an open enrollment that will be smooth and will increase the rolls of the insured,” said Maydad Cohen, special adviser to the governor on project delivery, who is leading the state’s recovery from the website’s failure a year ago. “We have high confidence that the system will work.” Although he added that there will definitely be some “bumps in the road” as with any website launch. In an interview, Cohen said the Connector had conducted 2,000 tests of the system, using fictional cases of people seeking health insurance. Only 105 defects occurred. Of those, 13 were “critical” errors -- either giving the wrong result or preventing the user from moving forward. An additional 47 were high-priority problems. While those 60 serious defects must be corrected, so far they can be fixed with relatively minor changes such as rewriting a line of code, Cohen said. He contrasted the situation today with the same time last year, when the state’s efforts to upgrade its website to comply with the Affordable Care Act went disastrously awry. “One thing we learned from last time,” Cohen said, “we don’t just rely on the word of our [technology] vendor to say ‘this will come tomorrow’ or ‘this will work.’ We get in there, we do our own testing. . . . We question, we challenge, we track. That kind of active involvement and relationship with our vendor is what helps also inspire our confidence.” Cohen expects to fix all major defects and stop the code-writing in late October or early November, moving into the performance-testing process to ensure the site will be able to manage high volumes of traffic. He expects the site to be able to handle 46,000 users at the same time on the first day of enrollment. Meanwhile, the Connector has hired 680 customer service representatives, more than double the number last year. The state’s chapter of the health care advocacy group Health Care for All (HCFA), recently weighed-in on their blog “We fully agree. We've seen live working demos of the site as well, and we're optimistic, too.”
-See the full Boston Globe article...
Psychiatric Appointments Difficult to Get in Boston This probably won’t come as much of a shock, but according to a new Harvard study, many people in large cities including Boston have a hard time getting an appointment for psychiatric care, even if they have private insurance. For the study, the researchers called 360 psychiatrists offices in Boston, Chicago, and Houston, who were listed in the Blue Cross Blue Shield online database and posed as insured patients or patients willing to pay out of pocket and attempted to get an appointment. The researchers were unable to obtain an appointment 75 percent of the time. An estimated 15 percent of the clinics were not accepting new patients; psychiatrists’ offices did not return phone calls 23 percent of the time; and 16 percent of phone numbers listed in the database were wrong. Psychiatrists in Boston were less likely to offer an appointment compared to those in Houston, the researchers concluded. The findings highlight the need for insurance companies to offer better access to mental health care by providing correct information about specialists in the area and whether they are accepting new patients, they wrote. -See the full Boston Globe article...
Officials warn of dangers of N-Bomb – A Synthetic LSD State officials are warning about a dangerous new synthetic drug that mimics the effects of LSD and has killed nearly two dozen young people nationwide in the past four years. The drug, known as N-Bomb, has been blamed by the U.S. Drug Enforcement Administration for at least 19 overdose deaths in California, Louisiana, Minnesota, North Dakota and Virginia between March 2012 and last November, when the federal agency classified it as a controlled substance. In Massachusetts, law enforcement officers have confiscated N-bomb but haven’t been able to pursue its dealers. The drug's compounds are not prohibited under current state law. A proposed law seeks to reclassify the drug and make it illegal. Rep. Cory Atkins, D-Concord, who filed the legislation, said N-bomb has become popular among teens and has been found by law enforcement in Chelmsford, Weston, Action and other communities. Erin Valentine, of East Bridgewater, said her 14-year-old daughter, Emily, died on June 24 at Massachusetts General Hospital of organ failure from an overdose of toxins that were in drugs she took three weeks before getting sick. Valentine said the hospital couldn’t determine what caused the overdose, and because of that State Police didn’t investigate her death. But she is convinced her daughter died as a result of ingesting N-bomb, based on conversations with her friends and text messages she sent about trying the synthetic drug. “Her life is gone because of a $5 hit of a drug that isn’t even illegal,” Valentine told lawmakers at a recent hearing. “This drug is on our streets and in our towns.” -See the full Eagle-Tribune article... For-Profit College Students Face Debt, Unmet Promises The pitch made by for-profit colleges, a staple of daytime and late-night TV, often features successful alumni from the schools, from Pulitzer Prize-winning photographers to Hollywood animators. Yet the US Department of Education estimated that 72 percent of the for-profit programs at 7,000 schools produced graduates who on average earned less than high school dropouts. Many of those students — veterans, single mothers, teenagers — end up in debt, often without degrees, jobs, or prospects. The practices of for-profit colleges have come under scrutiny in recent years, prompting federal and state investigations, lawsuits, and enforcement actions. The US Consumer Financial Protection Bureau in September sued Corinthian Colleges, alleging that the nation’s largest for-profit chain engaged in predatory lending. Corinthian officials said the lawsuit ignores evidence that thousands of its graduates are hired by employers every year and called problems cited by the agency “isolated incidents.” In Massachusetts, Attorney General Martha Coakley is investigating about a dozen for-profit schools, suing several, and has issued regulations to govern the industry. But the Massachusetts Association of Private Career Schools challenged her in federal court, alleging that the regulations are “unnecessary and unwarranted” and that she overstepped her authority. Industry advocates say for-profit schools help students who are squeezed out of oversubscribed community colleges and might not otherwise have opportunities for higher education. They argue that federal and state authorities impose a double standard— many students from nonprofit institutions also leave school burdened by onerous debts and without degrees and jobs. Students at for-profit colleges graduate at about half the rate of students at public and nonprofit four-year colleges and universities, according to the Education Department. The most recent data show that about 34 percent of students at for-profits earned bachelor’s degrees after four years, compared to about 55 percent for public institutions and 65 percent for nonprofit schools. Bachelor’s degree programs cost about 20 percent more at for-profit schools than flagship public universities, a 2012 US Senate committee report found. Associate’s degree and certificate programs at for-profits cost at least four times more than at community colleges, the report found. Students at for-profit schools default on federal student loans at higher rates, according to the Education Department. The department later this year will unveil new regulations aimed at preventing alleged abuses in the industry. The Association of Private Sector Colleges and Universities, the industry trade group, did not respond to repeated requests for comment. -See the full Boston Globe article, including in-depth case studies... 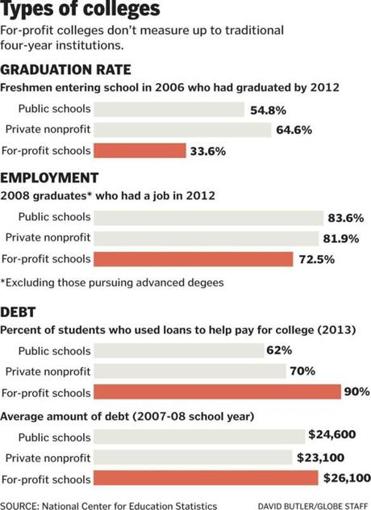
New 3-Minute Test Accurately Detects Delirium About 30 to 50 percent of hospitalized elderly patients will experience delirium at some point during their hospitalization, yet two-thirds of them go undiagnosed, raising their risk of life-threatening falls, pneumonia, and pressure skin ulcers. That’s because the standard screening for delirium — a state of severe confusion and disorientation — takes 60 to 90 minutes and involves questioning the patient, hospital staff, and caregivers as well as reviewing the patient’s medical chart. A new three-minute screening test for delirium, however, could soon become routine after researchers from Beth Israel Deaconess Medical Center determined that it’s nearly as effective as the longer “gold-standard” evaluation. In the study, published in the Annals of Internal Medicine, the researchers initially gave the longer assessment to 201 hospitalized patients, age 75 and older, and diagnosed delirium in 42 of them. The shorter three-minute assessment detected delirium in 40 out of the 42 patients and involved evaluating performance during a simple attention task, like reciting the days of the week backwards. The three-minute test also correctly identified 150 out of 159 patients who did not have delirium, which made it both sensitive enough to detect the condition and specific enough to avoid a high percentage of false diagnoses. Delirum, caused by high fevers, infections, or drug reactions, can often be mistaken for chronic dementia in elderly patients. A distinguishing characteristic of delirum is inattention — as opposed to memory loss, a hallmark sign of dementia. The screening helps doctors distinguish between the two. “About 80 percent of the falls that occur in hospital settings are related to delirum,” Marcantonio said. The resulting costs of managing sprains and fractures have created a major incentive for hospitals to prevent them since insurance companies have become more reluctant to reimburse for treatment related to hospital injuries. Marcantonio said he hopes the study’s validation of the three-minute assessment will enable delirium screening to become routine for older hospitalized patients, but whether or when that will occur remains unknown. -See the full Boston Globe article... |